Robotic Surgery

Endoscopic surgery is no longer considered a subspecialty, as laparoscopy is now the preferred method for every gynaecological condition, except for very few cases of oncology ,while it has replaced open surgery entirely, as it offers nothing but advantages. Robotic surgery is the evolution of laparoscopy and it is estimated that it will soon replace it completely as well.
The well-known advantages of minimally invasive surgery (laparoscopy), such as shorter hospital stays, less blood loss, fewer adhesions and lower patient mortality compared to open surgery, have been largely observed in robot-assisted surgery. Three-dimensional technology with improved dexterity up to 7 degrees of freedom and stable handling allows for better surgical field exposure in complex procedures.
The Da Vinci robotic system is equipped with an advanced computer platform, which allows the device's arms to move with absolute precision simultaneously with the operating table. As the endoscopic camera can be used on all four trocars, the device allows the surgeon to perform upper abdominal procedures, such as para-aortic lymphadenectomy or endometriosis removal from the diaphragm, with ease.
The combination of a well-trained surgeon and the capabilities of the Da Vinci system offer the possibility for detailed reconstruction of tissues, nerves, vessels, etc., thus performing the most difficult procedures with absolute precision.
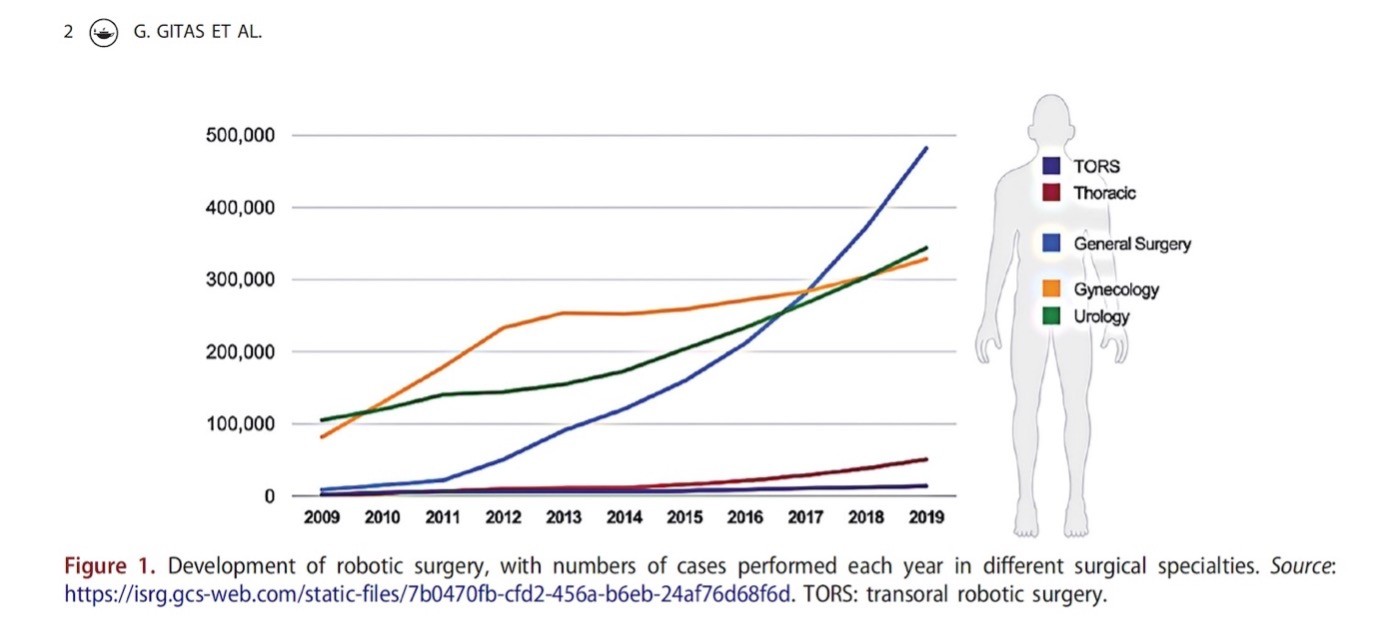
The scope of robotic surgery has expanded significantly since the da-Vinci robot was approved by the US FDA in 2005. In the United States, the use of robotic-assisted surgery increased from 1.8% in 2012 to 15.1% in 2018. Robotic hysterectomy is the most common robotic-assisted procedure in gynaecology, and the second most commonly performed procedure, second only to C-sections.
Existing studies show that patients who underwent surgery with the Da-Vinci device had excellent results in terms of quality of life and were very satisfied with their decision to undergo robotic-assisted surgery.
Especially patients with increased weight seem to have an exceptionally good outcome with the use of robotic surgery. Obesity, which has become an epidemic in developed countries, does not appear to be associated with a higher risk of mortality in patients undergoing robotic-assisted gynaecological surgery, unlike other techniques. This becomes particularly important as extreme obesity, expressed as a body mass index (BMI) ≥ 40 kg/m2, has increased more than fourfold since the mid-1980s and is now a major problem. The Da Vinci Xi device uses longer trocars, which are lifted by the robot arms allowing the surgeon to operate with less intra-abdominal pressure, which can reduce patient mortality.
Robotic Surgery with the Da Vinci system offers us absolute precision in the surgical handling of complex gynaecological procedures, such as difficult hysterectomies and removal of large uteri. Also, infertility problems in couples, due to endometriosis or adhesions from a previous infection, which require salpingoplasty, can be treated with absolute precision to obtain perfect results. We can now remove large and multiple uterine fibroids using advanced techniques.
In the field of urogynaecology, with the help of robotic surgery, we are applying innovative techniques such as pectopexy and Burch using natural tissues or synthetic meshes, and these techniques are coming to solve problems that plague women such as prolapse and incontinence. Even anterior vaginoplasty, i.e. bladder repair in the condition of cystocele, can be performed robotically, without incisions in the vagina, a technique that is carried out in a few centres abroad worldwide. A key point in the treatment of these patients is the correct diagnosis of the lesion and targeted treatment by choosing the appropriate surgical technique, which requires knowledge, experience and surgical skill.
Regarding gynaecological cancer, in certain large countries abroad, the specialised gynaecological oncologist is the only person qualified to treat patients with breast, ovarian, uterine, vulvar, cervical and vaginal cancers, as it is proven that this improves the survival rate and the chance of complete recovery of patients.
In the treatment of these diseases it is very important that the treatment plan is designed by experienced gynecological oncologists and in case of surgical treatment, specialized techniques should be used.
For the treatment of patients with endometrial cancer, the Da Vinci Xi device features the Firefly system that allows the surgeon to evaluate the patient's pelvic lymph nodes using indocyanine green (ICG) to find the sentinel lymph node and remove it instead of performing a full pelvic and para-aortic lymphadenectomy, thus reducing the risk of complications and post-operative lymphedema. This complication can occur either a few days after, or years after the surgery for lymph node removal, with chronic swelling in the legs. The more lymph nodes removed, the greater the risk of developing lymphedema. It has been reported that 37.4% of patients who underwent radical lymphadenectomy for endometrial cancer developed lower limb lymphedema. In some cases, lymphedema requires additional surgical treatment.
The major disadvantage of robotic surgery is that it is significantly more expensive than conventional laparoscopy. The authors of a Cochrane review, published in 2012, concluded that robotic surgery is significantly more expensive than conventional laparoscopy. However, the published cost assessments did not include the cost of complications, length of hospital stay and return to a normal routine after robotic-assisted or other surgical approaches.
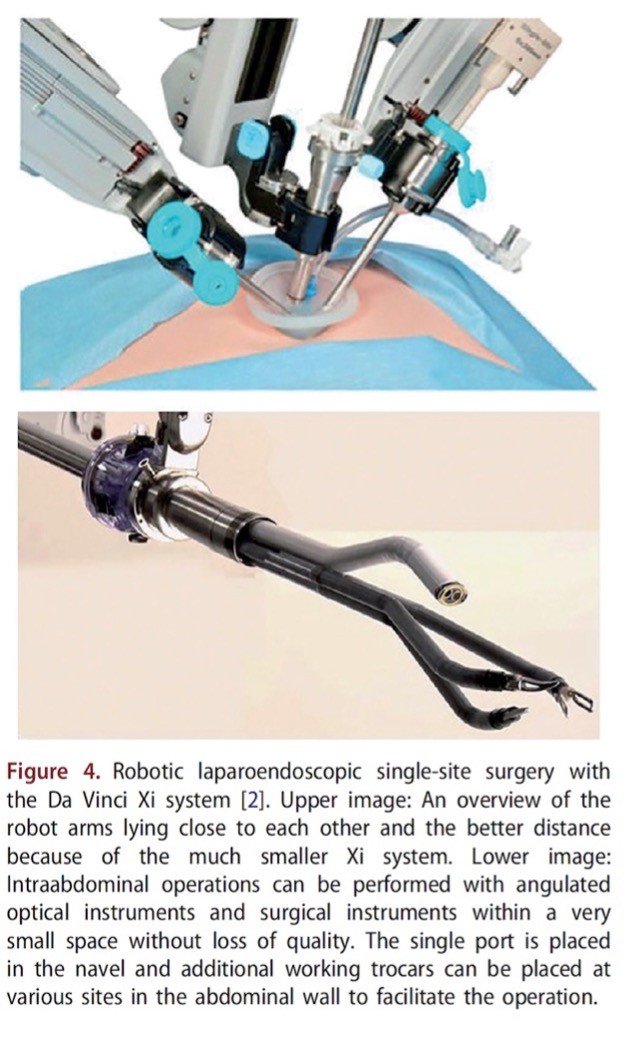
Robotic surgery in gynaecology through a single incision (R-LESS) was first performed in 2010. The GelPort system is placed in the umbilical region through a 2 cm incision. Postoperative hernia rates are comparable to other minimally invasive techniques. The development of this single-site technique can offer significant advantages for patients.
George Gitas is officially certified to use the Da Vinci system by its parent company Intuitive. Mr. Gitas was for many years, the director of the Endoscopy Center at the University Hospital UKSH Lübeck, Germany, performing complex procedures using robotic surgery. He then served as director of the Gynaecology Centre at the Charité Campus Mitte University Hospital in Berlin, where he introduced robotic surgery in the gynaecology department.
Mr. Gitas gives courses in endoscopy and robotic surgery at the School of Gynaecological Endoscopy at Kiel University in Germany, the renowned centre that gave birth to laparoscopic surgery, with the aim of passing on his knowledge to colleagues.
At the present, he is the director at the department of Gynecology-Robotic Surgery of European Interbalkan Medical Center.

